Laterally Stretched Flaps
Copyright © 2018 Instituto Carranza, Buenos Aires
The Laterally Stretched Flap™ is a surgical technique developed by Prof. Dr. Nelson Carranza and his team at the Carranza Institute (1). It is aimed at reducing the exposed portion of the graft, increasing its vascular supply and stability.
It comprises three main technical variants, the Laterally Stretched Tunnel Flap, the Laterally Stretched Envelope Flap, and the Laterally Stretched and Coronally Advanced Flap.
Before beginning
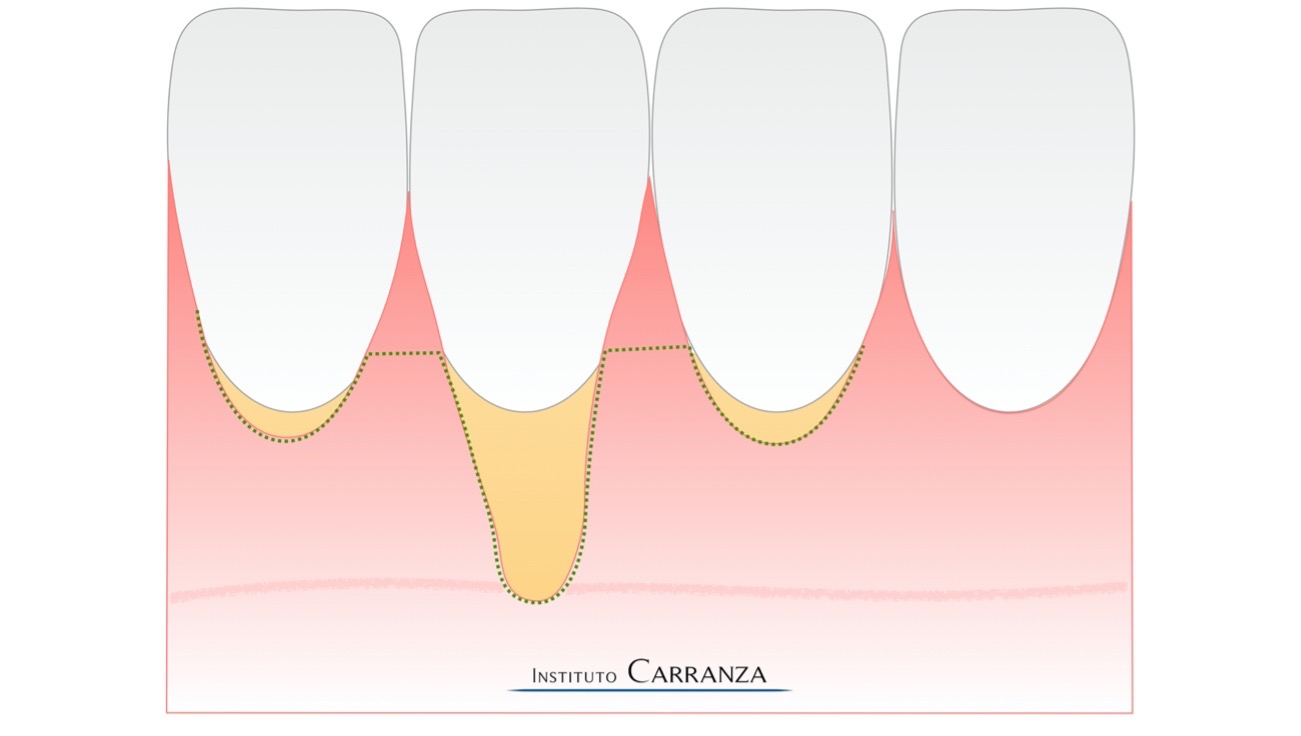
Determine the tooth or teeth to be treated. Maximum is limited by the expected lenght of the graft. Usually one to four lower anterior teeth are treated simultaneously, though only one or two deep recessions will receive the laterally stretched flap, while the remaining adjacent recessions will be treated with a non-displaced (tunnel/envelope) approach or a coronally advanced flap.
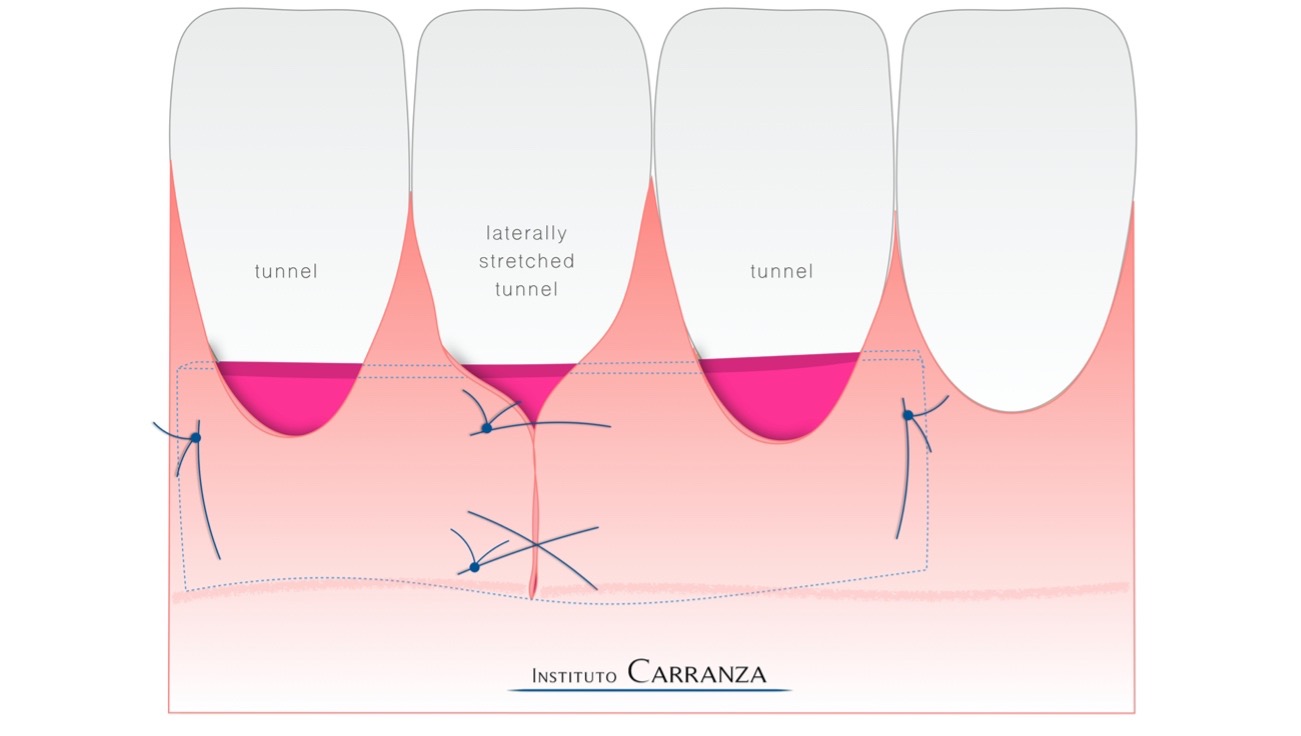
Laterally Stretched Tunnel Flap
This variant is based on the traditional tunneling techniques (2-3):
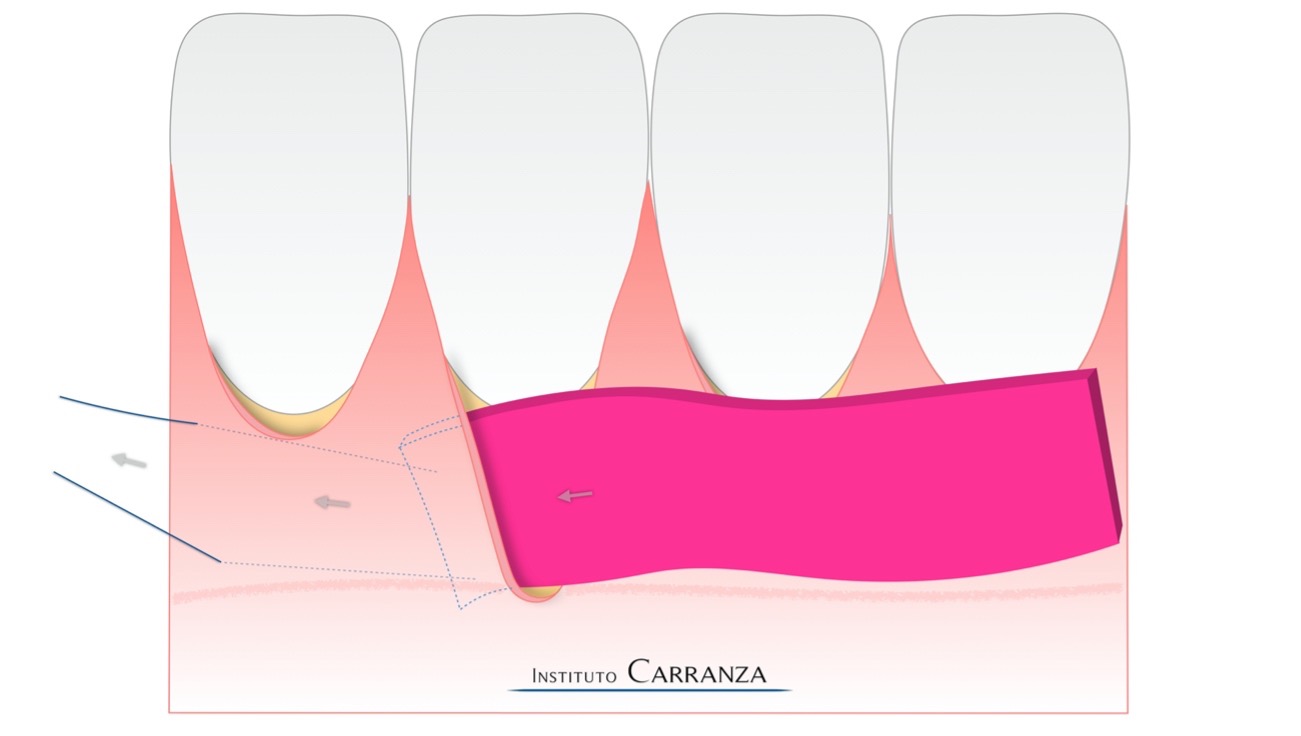
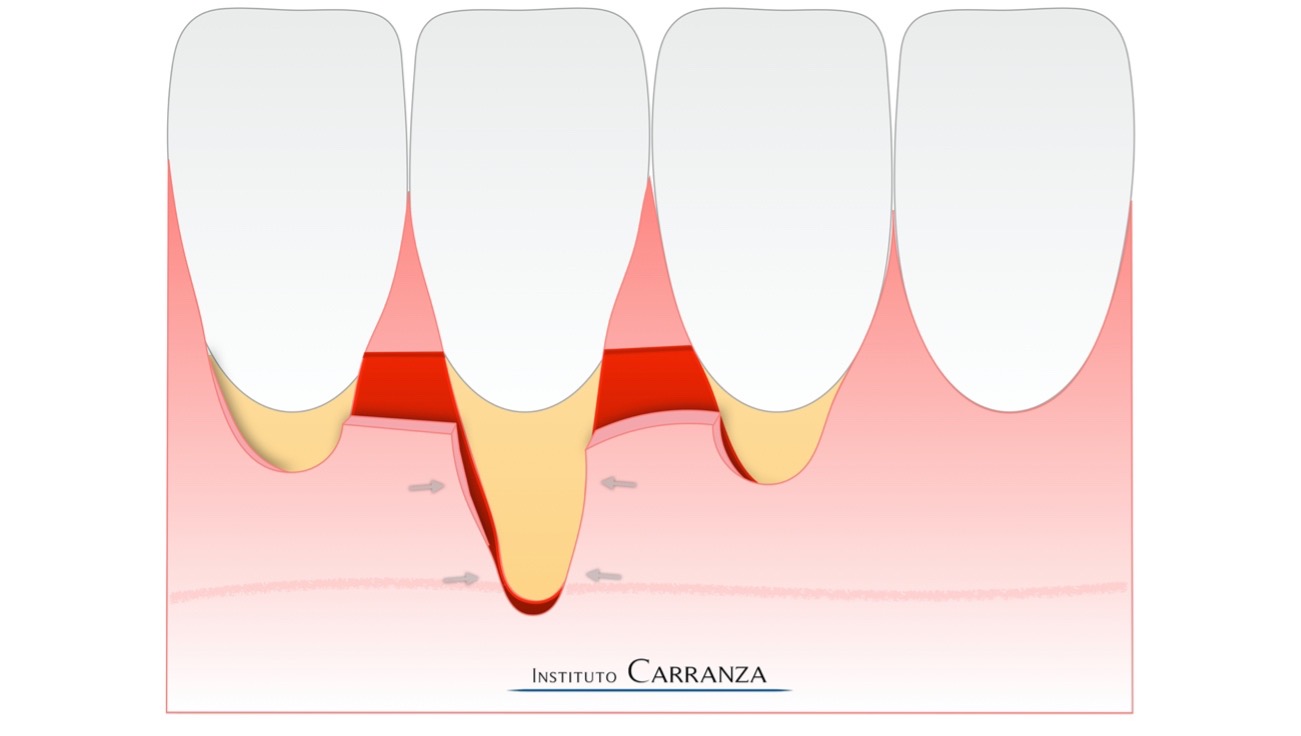
1) After intracrevicular incisions are made, a partial thickness tunnel is prepared with tunneling instruments. Facial areas of thin tissue, especially around the recession to be stretched, should be elevated in a full thickness fashion to ensure flap integrity and resistance. The tunnel should extend more than 5 mm laterally and apically until suffucient stretching can be achieved by gently moving the tissues with an atraumatic tissue plier. Beyond the mucogingival junction, a partial periosteal release may be accompanied by a partial submucosal release to liberate muscle tension from the flap. Root surfaces are planed and treated with EDTA for 60 seconds.
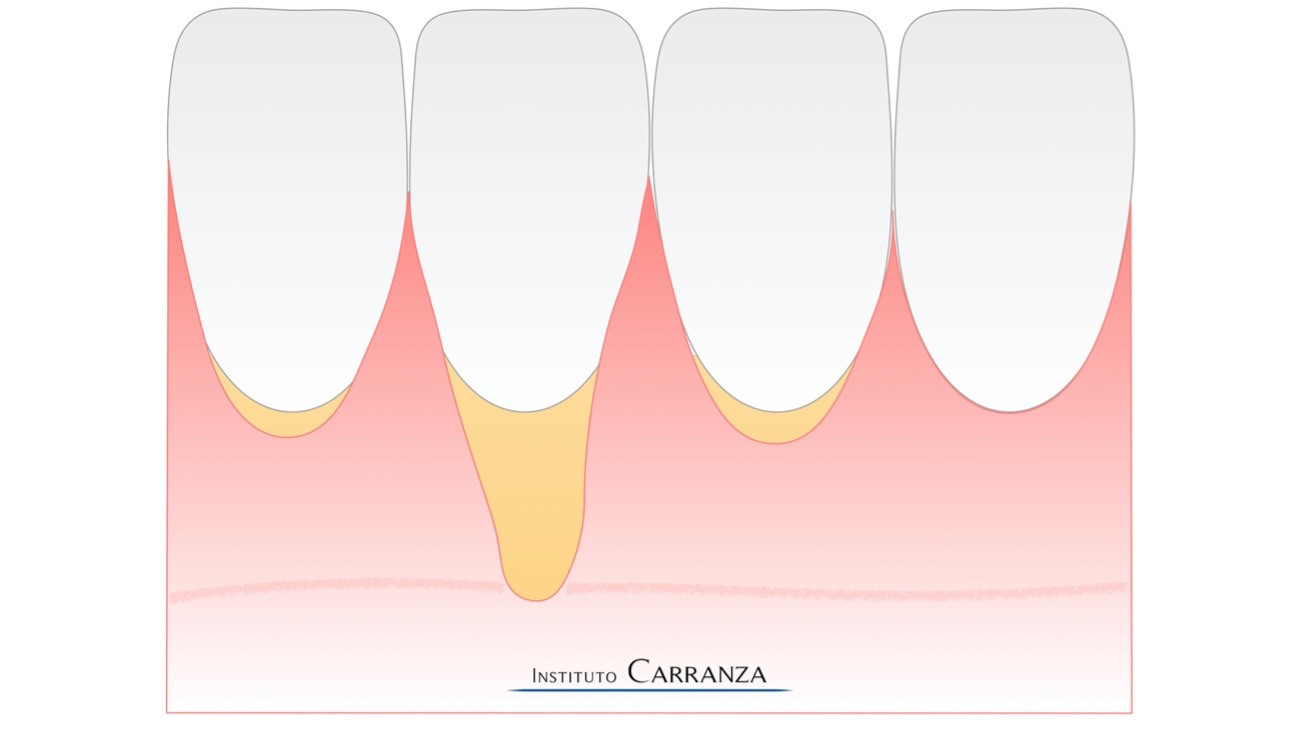
2) A graft of sufficient length to cover all teeth to be treated should be harvested from the palate. The graft is harvested following the Carranza’s Double Blade Grafting Concept (4), which ensures a predictable and homogeneous width of 1mm or 1.5mm.
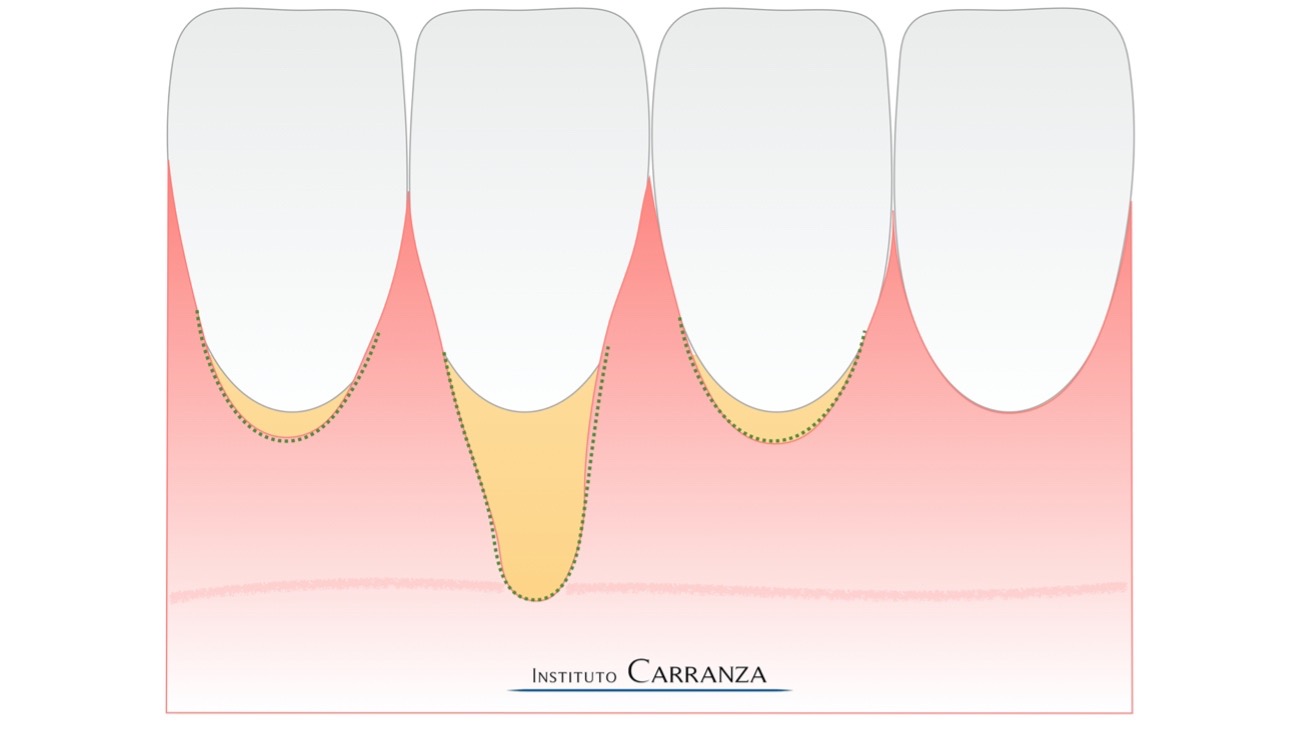
3) The graft is inserted into the prepared envelope with sling sutures in the usual manner, and secured at both ends.
4) The anchoring sutures shall be left with some slack to allow the lateral displacement of the tunnel flap.

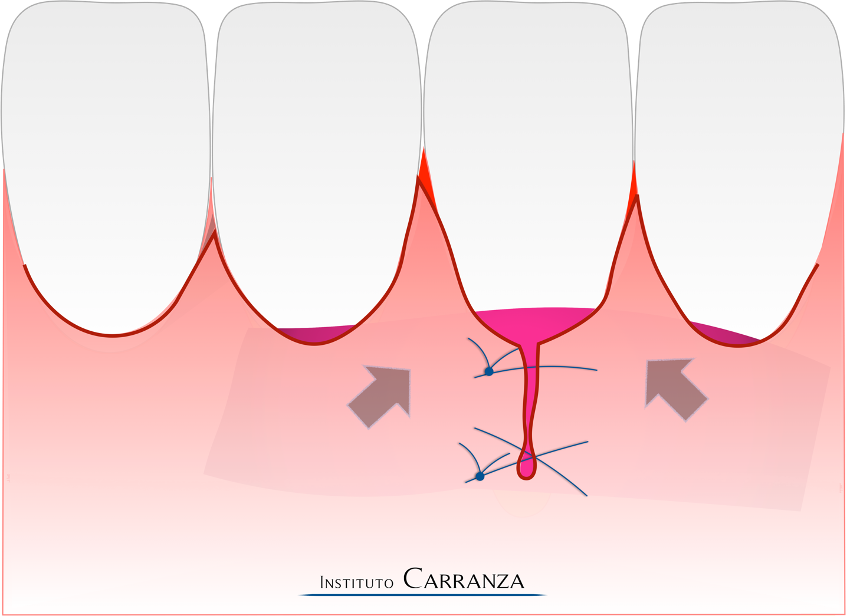
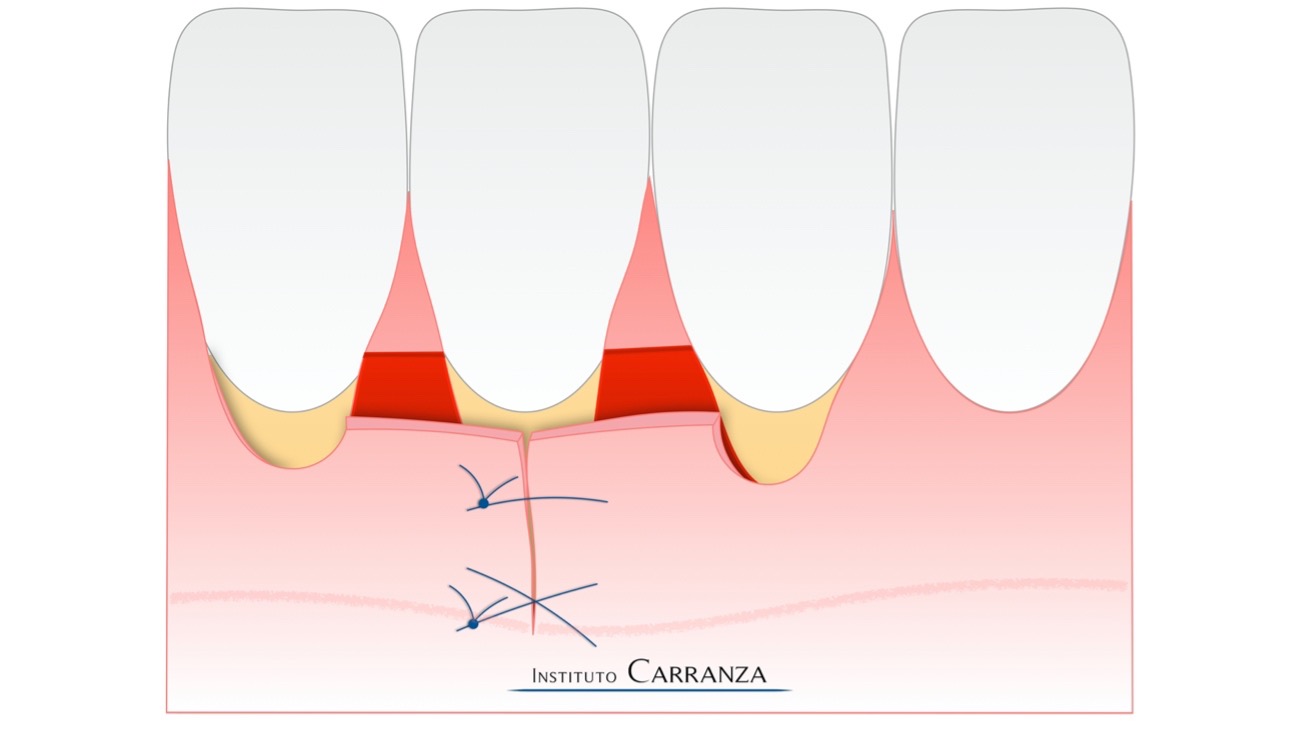
5) With the graft secured in its position, lateral stretching of the flap is performed with double-cross and/or simple sutures beginning from the apical extent of the recession and preoceeding coronally. Care must be taken that the needle only engages the flap but no the graft. Sutures are left in place 15 to 20 days post op.
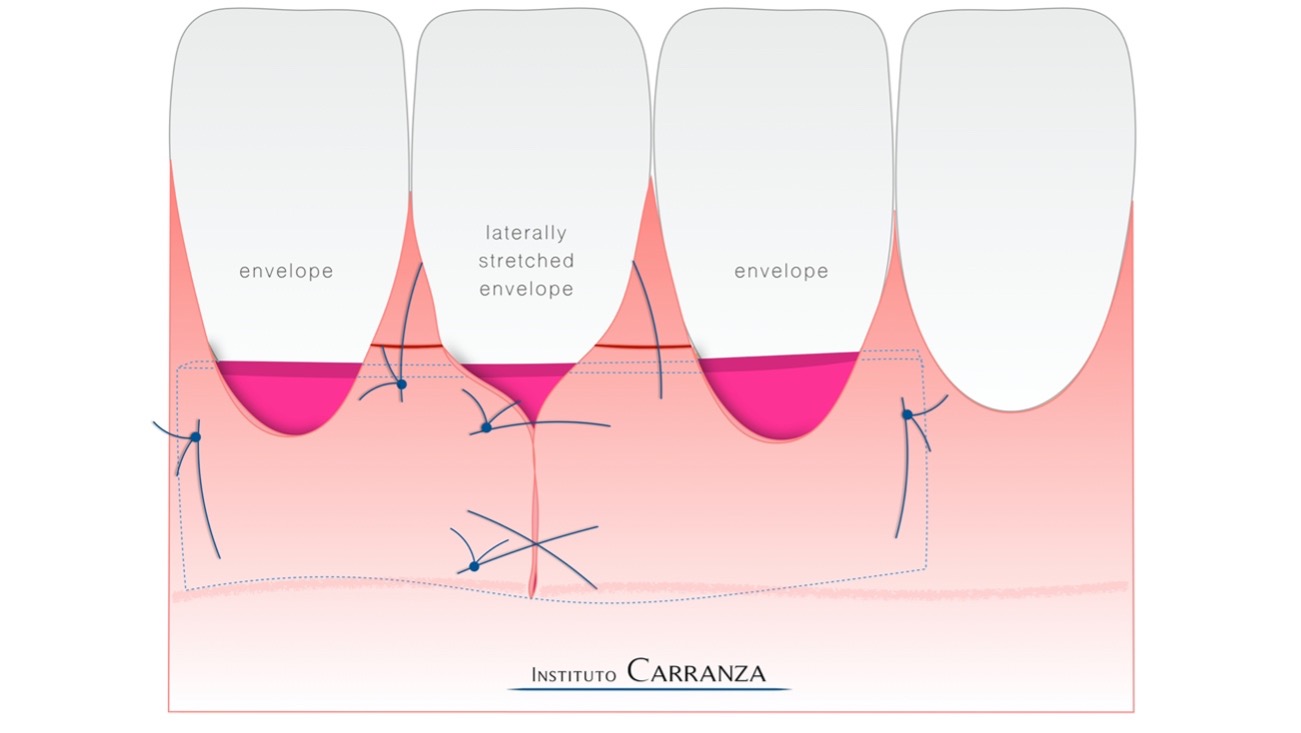
Laterally Stretched Envelope Flap
The Laterally Stretched Envelope variant is based on the traditional envelope flap technique (5). It was originally developed to treat deep/narow Miller class 3 recessions, but can be applied very successfully to Miller class 1 and 2 recessions.
1) Intracrevicular incisons are made involving the teeth to be treated, and connected interdentally by a horizontal incision at the base of the papillae.
2) A partial thickness envelope flap is elevated using tunneling instruments. Facial areas of thin tissue, especially around the recession to be stretched, should be elevated in a full thickn fashion to ensure flap integrity and resistance. The envelope flap should extend laterally and apically until suffucient stretching can be achieved by gently moving the tissues with an atraumatic tissue plier. Beyond the mucogingival junction, a partial periosteal release may be accompanied by a partial submucosal release to liberate muscle tension from the flap. Root surfaces are planed and treated with EDTA for 60 seconds.
3) Recipient bed is finalized by stretching the flap towards the deep/narrow recession and securing it with double-cross and simples sutures.
4) A graft of sufficient length to cover all teeth to be treated should be harvested from the palate. The graft is harvested following the Carranza’s Double Blade Grafting Concept , which ensures a predictable and homogeneous width of 1mm-1.5mm.
5) The graft is easily inserted into the prepared envelope. Holding sutures may be placed at the ends of the graft, but sufficient slack should be left to allow lateral flap displacement.

6) The graft is sutured altogether with the flap with a sling suture. This suture can involve one tooth (two papillae) or several teeth. The needle enters from the buccal side engaging the flap-graft-papilla complex, and exits through the base of the lingual papilla surrounding the lingual aspect of the tooth to engage the other papilla in a similar manner.
Laterally Stretched and Coronally Advanced Flap
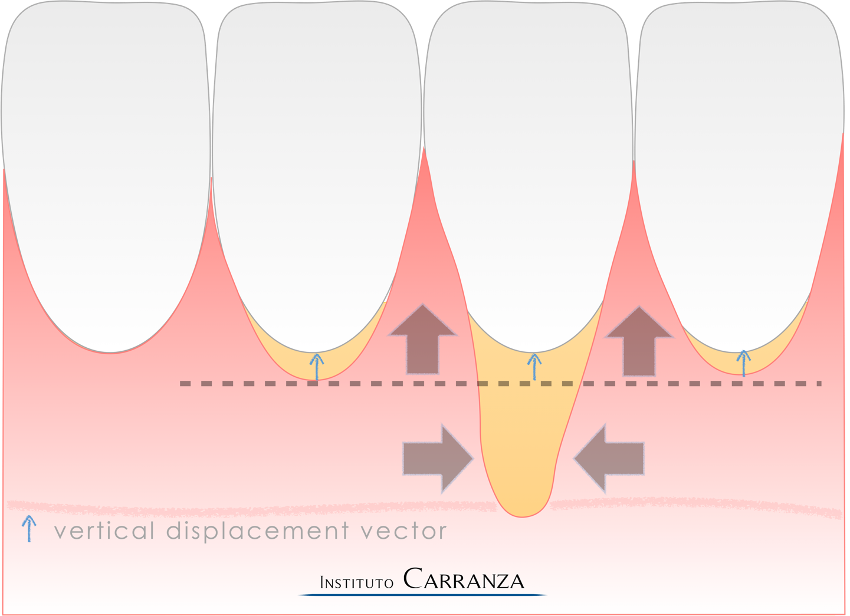
The Laterally Stretched and Coronally Advanced Flap variant is based on the traditional coronally advanced flap (CAF) technique (6). It is specially indicated to treat deep-wide single recession or multiple deep-narrow gingival recession defects. The objective of the LAST-CAF is to cover the graft in its most apical portion by performing a lateral stretching, while the most coronal aspect is covered by a complementary coronal displacement of the flap.

1) Determine the vector of coronal displacement. If adjacent recessions of lesser depth exist, a vector of displacement is established so that these recessions are fully covered by the coronal displacement. This vector is transported to the main recession defining a horizontal dividing line of displacement, the apical area will be laterally stretched, while the coronal area will be coronally advanced.
In cases of multiple adjacent deep-narrow gingival recession defects, the vector of coronal displacement is arbitrary defined.
2) Determine the design of the interproximal horizontal incision. In cases of papillae sufficiently wide and not overly blunted (RT1 and incipient RT2 recession defects), an oblique interproximal incision is indicated. Conversely, when the shape of the papillae is very narrow (such as in the lower anterior area) or blunted (RT2 and RT3 recession defects) a trapezoidal papillae design is considered more appropriate.
3) Once the interproximal design is determined, the vector of coronal displacement is outlined over each papilla adjacent to the deepest recession. In cases of triangular papilla design the oblique incisions are made diverging from the tooth with the deepest recession, in a reversed mode than as described for traditional CAF.

In cases of trapezoidal papilla design, two horizontal incisions are done: the first one is made 1 mm apical to the tip of the papillae and represents the end limit for the coronal advancement of the flap. The second horizontal incision is performed at the base of the papilla, coinciding with the apical end of the vector of coronal displacement.

4) The interproximal incisions are followed by intrasulcular incisions and a partial thickness envelope flap is elevated using tunneling knives. Facial areas of thin tissue, especially around the recession to be stretched, are elevated in a full thickness fashion to enssure flap integrity and resistance. Beyond the mucogingival junction, a partial thickness periosteal release is performed together with a periosteal release to liberate muscle tension from the flap until sufficient stretching and coronal displacement is achieved. Then, papillary areas coronal to the interproximal incisions are gently de-epithelialized. Root surfaces are planed and treated with EDTA for 60 seconds.
5) Finally, the recipient bed preparation is finalized by stretching the flap around the deep recession, in an apico-coronal direction, securing it with double-cross and simple sutures in the area apical to the dividing line of displacement.
6) A graft of sufficient length to cover all teeth to be treated should be harvested from the palate. The graft is harvested following the Carranza’s Double Blade Grafting Concept , which ensures a predictable and homogeneous width of 1mm-1.5mm.
7) The connective tissue graft is immediately sutured to the recipient bed with absorbable suture material.
8) Finally, flap suturing is performed. Sling sutures are placed at each one of the teeth involved in the surgery beginning from the periphery and advancing centrally to the laterally stretched recession.