I remember when the double blade knife was the latest novelty. Pretty much around the time Randall Harris (its inventor as far as I know) published his article in 1997

As many others, I ran to buy my double blade knife in the hope my grafting will be more precise, safer, and predictable. It looked so easy after all!
I guess my experience was similar to many others’. If the palatal vault was high, a decent graft could be harvested. But when I tried using it in medium-to-shallow palates, the inner blade hit the bone to soon, rendering a useless, short piece of «palatal tissue». Even worse, the grafting site was damaged beyond possibility to harvest anything from there. So, after taking a deep breath I had to tell the patient that we needed to go to the other side of the palate to harvest the graft. Of course, this time with a more traditional and trustworthy technique.
For a short while, I insisted in improving the technique and tryied two or three shallow passes, re-inserting both blades into the previous incisions, each time going a bit deeper. The result: A messy, irregular, frayed graft!
I finally gave up trying and went back to the traditional, trustworthy and reliable «Single Incision Technique», described by Hurzeler and Weng in 1999. My double blade handle went forgotten into drawer.
A few years later, while working with my graduate students, I realized that harvesting the graft from the inner aspect of a slightly elevated flap, was an easier and safer way to perform the Single Incision Technique. So effective it was, that we still use this modified approach nowadays whenever we use this technique.

One day it occurred to me to use that old double blade with our modified approch to the single incision technique and Voilá! The Double Blade Presicion Grafting (DBPG) Technique was born. (First published in «Harvesting Connective Tissue Grafts from the Palate», Nelson Carranza https://books.apple.com/us/book/harvesting-connective-tissue-grafts/id948366622 )
More than ten years have past, and hundreds (likely more than 1000) of grafts have been successfully harvested since we began using the DBPG. The technique has been perfected to a such a level that it has taken away the uncertainty of graft harvesting from our plastic surgeries. Moreover, this approach lets us decide the size, thickness, and composition of the graft we desire, and harvest it accordingly. This is the reason why, despite I still use the single-incision technique (Hurzeler) and the de-epithelilalized free gingival graft (Zuchelli), most of my cases are harvested with the DBPG technique.
The Double Blade Precision Grafting Technique step-by-step
First, you need to acquire a double blade bard-parker handle. Nowadays, I almost exclusively use a handle that holds two blade with a 1 mm separation between them to treat gingival recessions. This provides me with a graft slightly thicker, of around 1.2 mm after harvesting. If I need a thicker graft, for ridge augmentation for example, I may use the 1.5 mm or the 2.0 mm handle.

5 steps to success
- After anesthetizing the area, make a horizontal incision 2.5 mm apical to gingival margins of the teeth with a 15 or 15c bard parker blade.
- Elevate a short full thickness flap of 3 mm to 4 mm approximately in order to allow exposure of the connective tissue area apical to the incision.
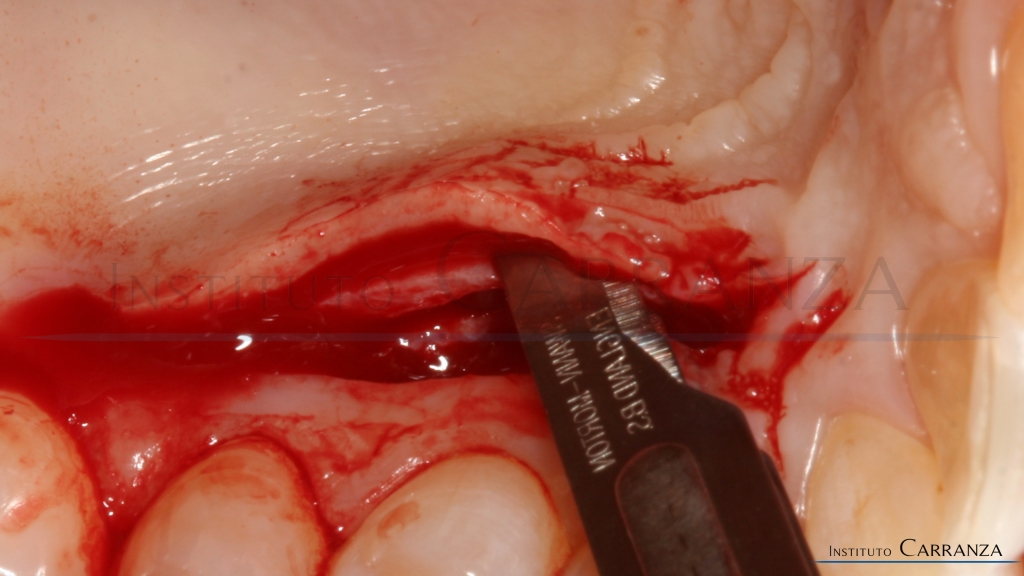
- Insert the double blade knife mounted with two bard parker 15 blades (not the 15c blades!- they are too thin and will bend) into the thickness of the detached palatal flap at its distal end. Take them to the desired apicocoronal depth, and then move slowly towards the mesial. The most superficial blade should should run about 1 mm away from the epithelial surface. If it runs closer, a denser graft will be harvested, but some flap necrosis will occur. If it runs deeper, more much glandular and/or fatty tissue will harvested.
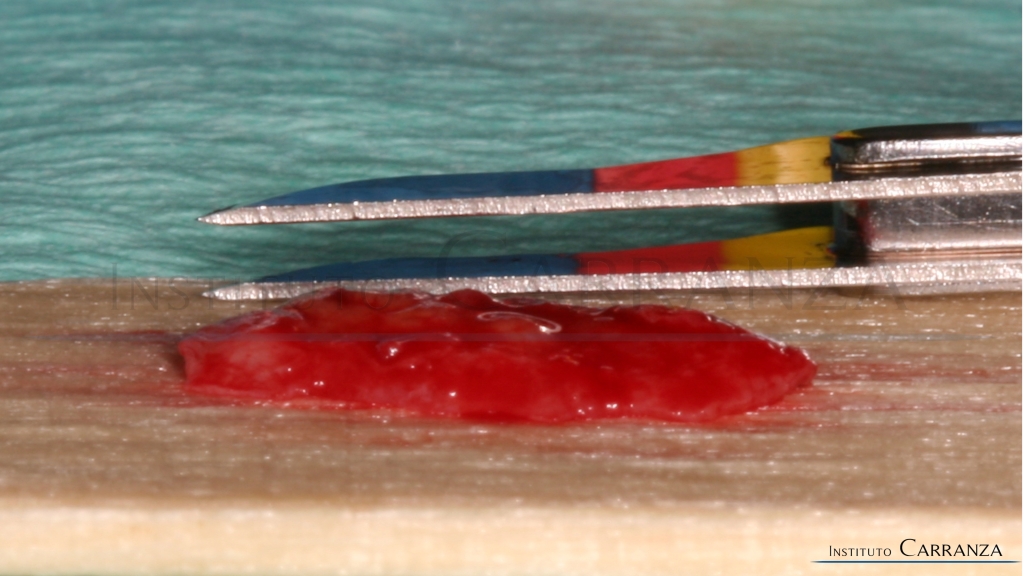
- Cut the perimeter of the graft with a mesial and a distal vertical incision, and a horizontal apical incision aimed to bony surface are made to liberate the graft. Special effort should be made to perform each one of these incisions in a single stroke to produce a distinct limit to the graft, and avoid tearing its edges.
- After the graft is extracted, primary closure is obtained with a double straight/crossed mattress suture.
final words…
It seems to me that the choice of harvesting technique has turned into a matter of taste. Most surgeons utilize one technique for all their cases. Lecturers advocate for a determined technique, sometimes very adamantly; histrionically. Somebody said once…»my graft is the best, and all others are sh@## grafts!». Do you like Italian or German?. Are we talking about cars???
You are probably comfortable with your current technique(s), and see no reason to change. But you are missing on something truly overreaching.
The DBPG adds a new set of advantages to the previous harvesting techniques which makes it very suitable in several cases. I understand, that it is not the best for beginners, but any one with some experience can do it. Of course, it requires a short learning curve, but I suggest not to give up before you mastered it. Then you can freely decide wether you like it or not.
We should feel confident performing every reasonable technique. The existing ones, and the ones to come. I personally utilize the single incision, the de-epthelialized free gingival graft, and the DBPG techniques. Each one provides a graft with different characteristics, and the selection of the technique depends on the requirements of each particular case. I believe that the choice should be based on the science, the skills, and the resources that will take you through the most predictable road to success, rather than just taste.
If it is a a matter of taste after all, you may join the great leagues of the «one technique surgeons», feeding yourself with the same soup everyday. But perhaps you want to add variety and true choice, and find you are a gourmet surgeon after all.
